[page 17]
Work of the Service
The duties of peripatetic teachers take them into hospitals, ENT and child health clinics, children's homes, schools and junior training centres. Each demands a different approach and different skills. Although not every teacher has responsibilities in every field, nevertheless many of them cover several. It cannot be expected that every individual will be equally skilled in them all; gifts and interests differ. Each field of work is considered separately below.
(i) Work in Hospitals
Several teachers of the deaf were employed by Regional Hospital Boards in Ear, Nose and Throat Departments as educational advisers. Although these people were not peripatetic teachers in the sense used in the survey and were not included in the investigations, their opinions were sought because they had a valuable contribution to make and their work affected that of the peripatetic teachers in the neighbourhood. Their main duties appeared to be assessment of the hearing of young children, preparation of audiograms for the otologists and consultants with whom they worked, early training of young children in communication skills and guidance of parents as well as advice about eventual school placement. In order to give useful and realistic advice it is essential for the teachers not only to know the home conditions in which the children live but also to have up-to-date knowledge of the available educational facilities in the area. Liaison with the local education authority is very important. This did not exist in every case.
Isolation from the educational system was seen to be a source of difficulty. In a hospital clinic it is possible, through enthusiasm and through incomplete knowledge of homes and schools, to make over-optimistic prognoses, to retain children on the books under clinic supervision for too long and to fail to pass on essential information to the education authorities whose responsibility they will eventually be. Because of this, local authorities are sometimes unaware of the presence of handicapped children in their areas; if such children come late to the notice of the peripatetic teachers outside the hospitals, suitable provision is difficult to arrange for them. Joint appointments by Regional Hospital Boards and Local Education Authorities largely avert this difficulty but are not without their attendant problems. Pressure from the otologists for the services of the teachers in preparing audiograms
[page 18]
and reports and following up children with significant hearing losses can upset the balance between the two sides and hospital duties may take precedence over work in homes and schools.
(ii) Work with Young Children in Clinics and Centres and at Home
Clinics outside hospitals were of two kinds: those which were set up for the one purpose of hearing assessment and which were frequently connected with special schools, and those which were part of the local authority's child and school health services. The former had the advantages of concentration of equipment in usually ideal clinic conditions and the proximity of a school with which the parents could become familiar. Work in local authority clinics afforded different advantages: it provided easy access to doctors and other medical staff and also gave the opportunity to discuss problems with health visitors, speech therapists and educational psychologists. Conditions in clinics varied; some were purpose-built, others were in old houses. Islanded amongst rickety card tables and the signs and smells of the previous night's social club activities, teacher and child in one 'clinic' managed to dismiss their surroundings from their minds in the concentration of intensive listening.
These clinics were attended both by young children brought by their parents and by children of school age. Some very young children who had failed screening tests were referred by health visitors: others were sent by otologists at local hospitals. Those children who were found early were likely either to be very deaf or to have disorders of communication or learning. The quality of reports upon such children and the information contained in them varied; as the teachers rely on them when, after re-testing, they undertake guidance of the parents and begin their home visits, it is important that they should contain full and accurate information. Re-testing the hearing of very young children is often difficult; through lack of special training, not all the teachers had sufficient skill and the results could be unreliable, especially when handling unresponsive children. Many teachers were concerned about children whose response was erratic or even lacking and who were later found not to be deaf. It was debatable whether they should have been included in their case loads. Many teachers had only limited knowledge of child development and needed additional training. In assessing the potential of children it is important to consider the whole child in his environment and learn to observe closely and record faithfully. Those who had attended the course in Advanced Audiology at Manchester University and who were also teachers of young children showed the value of their training.
In some cases guidance for parents was given only in the clinics. This no doubt saved travelling time for the teacher but it also had disadvantages:
[page 19]
if not handled with care the session could become a teaching period for the child rather than guidance for the mother. One grandmother who deputised for her daughter, was heard to say of a two year old. 'I've brought Tommy for his lesson'. It has to be made clear that these sessions are for the purpose of helping the parents of young children to understand the nature of their child's disability and its effects which include lack of normal means of communication. The teacher's role lies in convincing the parents that since facility in spoken English follows progressive stages and can be developed, they have an active part to play. Through purposeful guidance over a period parents can be encouraged to accept increasing responsibility for this growth of oral language and to make fewer demands upon the teacher's time. In this way, twice-weekly visits might be reduced to once a week and eventually perhaps to once a month. When this is achieved home visits might be replaced by sessions held at a clinic. It was seen to be much more difficult to achieve the right atmosphere in the clinic than in the homes where the children were surrounded by their own playthings and the mothers could be shown how to use the life of the home as a learning situation. Yet work in the homes was much more demanding: the mothers were more at ease in their own domains where the disciplined approach possible for the teacher in a clinic could not be enforced in the same way.
There were teachers who tended to 'teach' children rather than to help parents to develop their own skills. Some of them were conscious of their own lack of training and concerned that some of the mothers were unable to profit from guidance sessions. These mothers were living in over-crowded conditions, their families were large and noisy, they had other young children, or they could not grasp the significance of the advice. (Immigrant parents without an adequate knowledge of the English language were a particular problem). A mother who, on opening the door to the teacher, said 'Come in, sit down and keep quiet. You watch me this time' must have been like a bright star in a gloomy sky. She had accepted the guidance with understanding and knew her role.
Other factors also affected the time-table. Regular visits by men teachers to homes in some areas could be regarded with suspicion by unkind neighbours and lead to hurtful gossip. In these cases it was necessary to call in the evening; although this meant dealing with young children tired after an active day and upset the teacher's normal working hours, it had the advantage that other members of the family were at home and could be involved.
Home visiting with its purposeful guidance for parents can be the focal point of work with children whose hearing is seriously impaired. Since parents are usually in a highly emotional state and the peripatetic teacher's hand is the first to be extended in constructive help, his responsibility may
[page 20]
be very heavy. It is not an easy task to lead parents towards accepting a handicap that is so difficult to understand.
(iii) Work with School children in Clinics and Centres
Some teachers were concerned only with children of school age. The number of clinics and centres at which they worked influenced the pattern of their work. Only those who had one definite base with office, telephone, secretarial help and amenities for display and storage were able to make their rooms attractive to the children who came there. Others worked from many centres - one from as many as seventeen - and conditions were often far from good. Co-operation with medical officers at the clinics varied.
Teachers who were employed by or seconded to a school health service had some advantages, such as access to clerical help and their own accommodation in the school clinics. Perhaps because the appointment cards sent to parents were directives from the Principal School Medical Officer, the rate of failure to attend appeared to be low. Regrettably it seemed to be more difficult to make the service known and appreciated in the schools.
Children of school age as well as young children were referred to the teachers by some otologists; in one or two areas, it was evident that the otologists were using the teachers to provide themselves with a service. This was useful in some ways but the work involved could upset the general balance. Again, the quality of relationships and exchange of information between the teachers and the otologists and local authority medical officers was important. Some teachers were despondent about the lack of co-operation and complained of the paucity of information they received about children under treatment and those issued with hearing aids.
The main duties with children of school age were two-fold: assessment of hearing and improvement of performance in school. In most areas the hearing of all school entrants was tested; only eight teachers reported that this was not done. Screening and referring children to the teacher was done by specially trained nurses, health visitors, audiologists and clerical assistants.
A working group on 'the early detection and treatment of handicapping defects in young children' which was appointed under the World Health Organisation and met in November 1966 defined screening systems as implying the application to all children, 'of certain procedures which can be carried out in a short time by the less specialised members of the staff and which will give an indication of the presence or absence of certain disabilities. Some of these procedures may give a definite indication that the child either has the disability or cannot possibly have it. Others are less definite, indicating only
[page 21]
that the child may have a disability. If the result is positive, indicating the actual or probable presence of the disability, the child is referred for specialist investigation and care. If the result is negative, no further investigation is carried out.'
Screening of school entrants brought to light many children with slight hearing losses due to catarrhal conditions which might clear up in the normal process of growth. Indiscriminate follow-up of all these children involved teachers in much work that was not profitable use of their time. One teacher was reported to have 1,370 children on his register. Such a case-load precluded work in schools. The priorities determined by teachers with very large case loads were usually assessment of hearing (which they carried out at the request of otologists and school medical officers) and follow-up of screening tests. So many children were referred for assessment, following routine or selective medical inspections or after screening, that very little time remained for tutorial or remedial work. One teacher devoted nine sessions per week to assessment and one to school visits. This was in great contrast to the brief laid down at the commencement of the service in that area.
Children whose hearing loss constituted an educational hazard were referred back to the medical officers and otologists for further attention and possible supply of hearing aids and were kept under review. Those whose speech was poor and whose attainments indicated retardation were accepted for tutorial work in speech, auditory training and development of communication skills. Such work could be with individuals or with groups, in the clinics or in schools. Many other children, particularly those who lived in industrial areas, had intermittent periods of hearing loss which, although not severe at any one time, were nevertheless significant in total and gave rise to retardation in school work. These children are properly the responsibility of the ordinary teachers, who require information from the peripatetic teachers in order to understand the educational need in such conditions. Working in the clinics often afforded valuable opportunity for collaboration with speech therapists and educational psychologists. It saved travelling time but it tended to be divorced from the schools and normal educational practice. Where the significance of the work was not realised either by the family or by the school, it sometimes resulted in spasmodic attendance at tutorial sessions.
Related duties included recommendations for school placing and change of school. This demanded a knowledge of local and regional provision which not all teachers had; in some areas closer links between the peripatetic teachers and the schools, both special and ordinary were needed. Many children who were linguistically retarded required more help than the teachers had time to give. Many of the teachers were urging their local authorities to set up
[page 22]
units for the partially hearing, but in the present shortage of qualified teachers of the deaf to staff them, such pleas can be unrealistic.
The relationship of the peripatetic teachers with children admitted to partially hearing units varied. In some areas connection ceased when the children were admitted. In others, the teachers continued in an advisory capacity and maintained interest in the children's progress and their future school careers. For this kind of relationship it is essential that the function of the service is understood, that the peripatetic teachers are diplomatic, tactful and persuasive and that their status is accepted by the headteachers. That many of them possess such qualities was evident in those areas where relationships between them and the headteachers were good. The units are integral parts of schools and although the work done in them may be outside the experience of the heads, they come under their authority. For the peripatetic teacher whose status is not determined, giving guidance to inexperienced teachers in the units might be regarded by the heads as interference.
The same qualities are called for when recommending placement in special schools. There were very few instances of disagreement between peripatetic teachers and special schools or of parental objection to special school placement.
(iv) Work in Schools
The majority of children with impaired hearing had been identified through screening tests at the time of entry to school but some who had missed the screening tests in their early school life or whose deafness was later in onset were referred by school medical officers. On-going assessment was continued but, with the passage of years, duties became mainly educational with older pupils. Teachers were seen at work in nursery, infant, primary, secondary and special schools and in junior training centres. Each type of school set its own problems.
By virtue of their organisation, nursery, infants' and progressive primary schools appeared best able to use the service provided by the peripatetic teachers, although finding space for working was not always easy. Good co-operation with clear desire to give maximum help to the children was evident in many, and some peripatetic teachers were able to spend valuable time in the classrooms talking to the teachers and observing the children at work. In many schools where co-operation was unstinted, over-crowded conditions, noise and poor facilities for testing were unfortunate obstacles.
Since the visits made by teachers with heavy case-loads are likely to be infrequent, the value of time spent in tutorial work is doubtful. Half an hour per week (a generous allocation) is small in relation to a 25 hour school
[page 23]
week. It is important, therefore, that there shall be opportunity to talk to the class teachers and advise them about the disability and the handicap it can impose and about hearing aids, their uses, their limitations and their maintenance. In many schools, where classes were large and teachers were over-pressed, it was often difficult to find opportunity to talk in this way. The advisory function of the peripatetic service is carried out in some areas by means of one-day conferences to which groups of teachers from ordinary schools are invited. Such conferences should be arranged regularly and frequently in order to keep pace with staff changes.
Work in secondary schools presented the greatest difficulties. Pupils were taught by many different teachers, not all of whom were interested in the special needs of minorities, and opportunities for meeting those most involved were not easy to arrange. It was seldom that one teacher had responsibility for the handicapped pupils in general or for those who wore hearing aids. Additional help was needed in many subjects. For work of value to be done, this called for liaison with different specialist teachers in each school and demanded wide interests and knowledge. In large schools, some of which spread over several buildings on an extensive campus, there was the task of finding the pupils, finding a space in which to work and fitting the session into the peripatetic teacher's and the pupil's time-table. Much precious time was consumed in this way. It is doubtful if the services of peripatetic teachers, who are in short supply, are used economically in such remedial work in secondary schools. Part-time teachers interested in remedial work might be an alternative source of help.
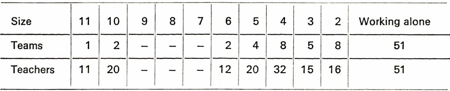
Workers in teams were able to specialise in specific subjects or certain ages but then had to cover larger areas. Some members assumed charge of young children while others attended to the older group; some, at secondary level, provided help in specific subjects. The problems inherent in allocating duties spread over large areas are matters of deep concern. Demands were greatest upon teachers working in isolation, who would, of necessity, have to cover all stages, all levels and all subjects. An organiser in one county arranged meetings and weekend conferences for his assistants and planned to invite teachers from neighbouring areas to join them.
A number of teachers went into junior training centres, where they were welcomed. Conditions were often difficult but the contact was worthwhile.
Some teachers referred to problems that arose from the frequency of staff changes in the ordinary schools; the same cause gave rise also to difficulties in the peripatetic service. Teachers who had worked consistently in one area had built up the confidence of headteachers and teachers in local schools, and the degree of co-operation was high. Conversely, in an area where changes were frequent, a full establishment had been reached in
[page 24]
only two of the thirteen years of its existence. It was impossible, in the resulting situation, to give a reasonable service. Stability is essential if work of any value is to be done.
(v) Liaison with Parents
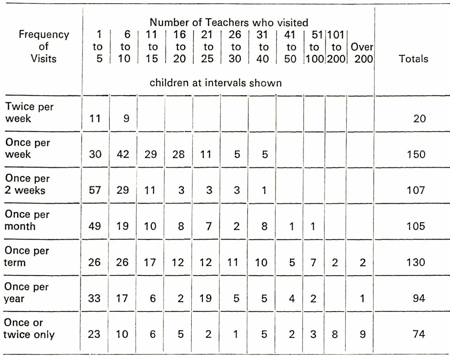
The size of case load held by the teachers was indicative of the kind of work with which they were faced. Although large numbers frequently included children who were seen only once, there were always some who needed continuous attention and whose parents appreciated guidance and support at all stages. Too often, guidance was given only when children were young. Parents, as well as their children, and the teachers, need to know about the use, value and maintenance of hearing aids. They need also to have contact with other parents similarly placed and to meet together to discuss their common problems. Those teachers who, along with parents, took active part in Parent/Teacher Associations and the National Deaf Children's Society and other appropriate organisations and those who organised day and weekend conferences were doing good work.
(vi) Liaison with other Services
The amount of liaison with other services differed according to the personality and opinion of individual teachers. Smooth-running services resulted when teachers pursued a firm policy of close co-operation with heads of special schools for the deaf and units for the partially hearing, with other kinds of special schools, with hospitals and with officials of the local authorities. It was unfortunate that in some areas where there was variety in provision and there could have been useful collaboration, liaison between the different workers was poor and opportunities for co-ordination were lost.
Children placed in boarding schools a long way from their homes are often lonely in the long summer holidays. Several peripatetic teachers, who had known boys and girls from the time when they were very young, organised social occasions for them and acted as a link between home and school. Knowledge of the background of pupils who live many miles distant can be very difficult to obtain and by way of this link with peripatetic teachers heads of special schools who understood the purpose of this aspect of the service were able to receive valuable information.
Since all except organisers had school holidays, such activities were not possible if the holiday periods coincided. Sometimes staggering of holidays allowed teachers still to be at work when the schools were closed. There
[page 25]
was, of course, no difficulty in Lancashire and parts of Yorkshire where school holidays coincide with Wakes weeks, which are staggered between towns.
From beginnings such as this, comprehensive organisations involving all services are slowly emerging.
(vii) Liaison with other Agencies
In a very few areas, liaison with other agencies was developing. Some of these agencies were part of the local authority health service: others were within the education department. Teachers who worked from health and school health clinics and were able to meet and discuss problems with medical officers, speech therapists, health visitors, social workers and personnel from child guidance clinics found this of great value. Others profited from their contact with educational psychologists and members of remedial teams. Each had a contribution to make in reaching decisions about suitable educational provision. Young people leaving boarding schools and entering employment needed support, advice and guidance on leisure pursuits and careers. Contact with Youth Club Leaders, Youth Employment Officers and Welfare Officers of the Deaf was useful. Several peripatetic teachers were becoming increasingly conscious of their role in maintaining contact with the young people until they were settled in their jobs. This applied not only to the leavers from boarding schools but also to those from day schools and units. Many pupils travel long distances to their day schools. In one case a peripatetic teacher ran a club which catered for their immediate needs and was fully appreciated.
Many young people leaving school had received no advice that they could understand as to how to find and pursue courses in further education and those peripatetic teachers who were knowledgeable and ready to guide them were fulfilling a valuable function.
In addition to their work with children and teenagers, many teachers were acting as advisers to local education authorities. This called for wisdom, vision, tact and knowledge. Not all had enough experience to develop these qualities or to give them the full knowledge of educational goals that are required for such responsible positions. Their plea was for enlightened leadership from people who understood not only the needs of children with impaired hearing but also the full extent of educational provision. Many of these general duties tended to be outside the scope of the normal hours of a teacher's working day and they called for a flexible time-table into which administration and clerical work could be fitted. The organisers were able to arrange their programmes according to demands; not all of them had case
[page 26]
loads. Their team members were differently placed: in many cases their duties had become too complex.
Peripatetic teachers cannot provide special educational treatment for all hearing-impaired children in their areas. They can only make recommendations for what they consider to be suitable provision and give definite help to a limited number whose handicap is not severe.
[page 27]
Priorities
Since the heavy demands imposed upon the teachers are not likely to be fully met by increased staffing for several years to come, it is necessary for appointing bodies as well as teachers to be clear about priorities. If there is to be full growth of this service terms of appointment must be related to the special skills of the teachers. Only in this way will maximum use be made of the teachers available.
Many case loads are unrealistic and the resulting services are a cause of dissatisfaction both to the teachers and to the local authorities employing them. Survey of the daily programmes, with their attendant problems, suggests that a redefinition of priorities is needed. The following are considered appropriate functions of a peripatetic teacher but the emphasis may vary according to local circumstances.
1. Collaboration
(a) with special schools and units catering for children with impaired hearing to provide a comprehensive service
(b) with other services
(c) with other agencies
2. Audiometric testing of hearing; sustained observation and assessment only of those children who are likely to need special education or additional help in school
3. Advice on educational placement based on full knowledge of the abilities and disabilities of each child under consideration and the facilities available in the area or region
4. Parent guidance as an on-going service
5. Training children in
(a) auditory discrimination that leads to optimum use of hearing aids in all situations
(b) auditory discrimination linked with improvement in speech and growth of language
(c) maintenance of hearing aids
6. Advice to teachers in ordinary schools
7. Remedial teaching that is closely linked to the work of the school and is limited to children whose need is for more specialised help than can be provided by an ordinary remedial service
8. Follow-up of children placed in schools and units remote from their homes.
[page 29]
Observations and Conclusions
The value of this service is evident. It can provide the focal point for the beginnings of education for children with all degrees of impaired hearing but it cannot provide a continuing full education for all of them. It can ensure that parents are given guidance in the early years when their emotional needs are at their height; it can give them continued support as their child enters each succeeding stage of development. It is a worthwhile service but is not as yet fulfilling the role of which it is capable. The following observations are offered as a means to further development.
1. The peripatetic teacher of the deaf holds a highly responsible position in relation to the educational provision that is made for children with impaired hearing. The children's future development can be determined by him. Continuity is an important factor in the establishment of a good service.
Appointments should be made with care and conditions of service should be such as to foster stability.
2. The superiority of a service in which medical and educational departments fulfil their roles in harmony is clearly evident. Liaison is much affected by quality of relationship and ease of communication between them. The peripatetic teacher has a significant part to play as the link between them.
In order to preserve the right balance between the two, the teacher appointed should have the personal qualities, the knowledge and the training needed for the post.
3. The advantages of a service in which peripatetic teachers have vital connections with colleagues, schools and other services and agencies are very marked. Work in isolation is frustrating and, in many cases, unsatisfactory and much time is wasted in travelling.
Area development is recommended, in which teachers work under the direction of a skilled leader or organiser, whose aims and personal qualities encourage positive linkage with other services.
[page 30]
4. Frequent communication is needed between members of a profession whose work is done in comparative isolation. Deterioration in quality of work, and diminishing sense of purpose, can occur when there is no opportunity to share ideas.
In developing plans for regional organisation, facilities should be provided for regular meetings in a central place where there is a good supply of up-to-date literature and text books and from which the work can be directed.
5. Demands for additional staff are not always reasonable. The service, as it develops, is mainly advisory and in many cases further consideration of the duties undertaken will lead to re-organisation of the programme and more economic use of the skills particular to teachers of the deaf.
The pressures on the specially qualified teachers could be reduced by re-examination of the duties involved, collaboration with remedial services and the appointment of part-time teachers (who are not necessarily qualified teachers of the deaf) to help with remedial sessions, particularly at secondary level.
6. Screening procedures for babies and school entrants are now general in the country. Time spent in testing five and six year olds who will not need the special skills of peripatetic teachers of the deaf upsets the balance of their work.
A second more searching screening test, carried out by workers other than teachers, would result in more appropriate cases being referred to the peripatetic teachers. Some additional training for this work would be required.
7. In some areas, maintenance of hearing aids and supply of spare parts is taken over by the peripatetic teachers of the deaf.
While the reasons for undertaking maintenance duties are understood, it is no part of the teacher's duty to spend time in making moulds for inserts.
8. Conditions in clinics and schools are not always easy. Those arising from physical difficulties cannot often be changed and must be accepted. Others arise from lack of understanding.
The purpose of the service and the status of the teachers should be made clear.
[page 31]
9. The different aspects of administration, both medical and educational, are a frequent source of worry to the teachers.
Short courses of training in administration would be of value to many teachers.
10. Many teachers regard work with young children as fundamental to their duties but few are fully confident even after several years of experience. Because their knowledge of child development is insufficient to enable them to differentiate between the normal and the abnormal, they are often uncertain about their conclusions. Testing, assessment and diagnosis and the beginning of training in the development of communication skills all present difficulties that are sometimes excessive.
A scheme of training in all aspects of pre-school work is urgently required. Many teachers now in the field would benefit from such a course.
11. Parent guidance is frequently orientated in the wrong direction and emphasises teaching the child rather than guiding the family. It is a broadly based subject that demands knowledge of family structure and characteristics, the influence of environment and the study of sociology.
A scheme of training to include parent guidance and all the allied aspects of sociology is needed.
12. When accepting responsibility for recommending placement in school peripatetic teachers do not always have full information on local, regional and national facilities. Standards in ordinary schools can be estimated by teachers who have had several years' experience in them but conditions and methods change and schools assume different characteristics with changes of head and staff.
Peripatetic teachers need to be up-to-date in their thinking. They should be given opportunity both to attend courses and to visit those educational establishments to which children in their care may need to go. Valid recommendations for placement cannot be made without up-to-date knowledge of facilities.
13. When young people whose hearing is impaired first take up employment, they very often need more support than their parents and the schools they have left can give.
The peripatetic teacher of the deaf can fulfil a role in giving support in the early period at work. (The teacher who is knowledgeable about
[page 32]
local conditions and opportunities for employment that is suited to young people with hearing impairment can be of particular value to the school leaver who is not in direct contact with a welfare officer for the deaf.) It will be necessary to make the purpose of this aspect of the work clear to head teachers, welfare officers of the deaf and youth employment officers.
14. The survey has shown that the peripatetic service is the starting point of the education of hearing-impaired children. All other branches of provision develop from it. The survey has also shown the wide range of roles and duties of the peripatetic teacher of the deaf and the difficulties which may arise in such a service, especially when teachers are working in isolation. The special skills of such teachers, who are in short supply, are used to the fullest advantage when they are able to work in close co-operation with others concerned with the education of hearing-impaired children in ordinary schools as well as in special schools and classes.
There is an obvious need for the development of comprehensive and closely integrated educational provision for all children with impaired hearing in which peripatetic teachers of the deaf can play their part in close co-operation with others.
[insert]
[The following type-written note on a sheet of paper was inserted at the back of the document.]
NOTE
The leaflet ("Teach Deaf Children") has been prepared by a group of the organisations concerned, in order that the interest and possibilities of this work can be brought to the attention of young people contemplating a teaching career. This leaflet, which gives an up-to-date and succinct account of the opportunities for training and teaching, is being distributed to colleges and university departments of education and to youth employment officers.
[inside back cover]
© Crown copyright 1968
Published by
Her Majesty's Stationery Office
To be purchased from
49 High Holborn, London WC1
13A Castle Street. Edinburgh 2
109 St. Mary Street, Cardiff CF1 1JW
Brazennose Street, Manchester M60 8AS
50 Fairfax Street. Bristol BS1 3DE
258 Broad Street, Birmingham 1
7 Linenhall Street, Belfast BT2 8AY
or through any bookseller
SBN 11 270031 4